DENGUE FEVER: OVERVIEW OF MEDICAL ACTIVITIES IN SRI LANKA
Fernando Hirunya
Scientific adviser: Ph.D., associate professor L. P. Mamchyts
Educational institution «Gomel State Medical University» Gomel, Republic of Belarus
Introduction
Dengue is a mosquito-borne viral disease that has spread rapidly in all regions in recent years.
Vectors of the dengue virus are female mosquitoes, mainly of the species Aedes aegypti and, to a lesser extent, Aedes albopictus. This mosquito also transmits chikungunya, yellow fever and zika infection. Dengue is widespread in the tropical and sub-tropical areas of the world, with local variations in risk largely dependent on rainfall, temperature, and spontaneous rapid urbanization.Severe dengue was first recognized in the 1950s during dengue epidemics in the Philippines and Thailand. Currently, severe dengue affects most Asian and Latin American countries and is one of the leading causes of hospitalization and death among children in these regions. Dengue usually occurs as epidemics in Sri Lanka following monsoon seasons.
The causative agent of dengue fever is a single-stranded RNA virus of the Flaviviridae family; there are 4 different but closely related serotypes of the virus that cause dengue (DEN-1, DEN-2, DEN-3 and DEN-4). After recovering from an infection caused by one of these serotypes, there is lifelong immunity to that particular serotype. However, cross-immunity to other serotypes after recovery is only partial and temporary. Subsequent cases of infection (secondary infection) with other serotypes increase the risk of severe dengue. Dengue is transmitted by the bite of an Aedes mosquito infected with any one of the four dengue viruses. Symptoms appear 3-14 days after the infective bite. Dengue fever is an acute flu-like febrile illness that affects infants, young children and adults. It can cause disease in two forms:
(a) Dengue Fever (DF) — marked by an onset of sudden high fever, severe headache, pain behind the eyes, and pain in muscles and joints.
Some may also have a rash.(b) Dengue Hemorrhagic Fever (DHF) — is a more severe form, seen only in a small proportion of those infected. Typically DHF is characterized by high continuous fever for less than 7 days; bleeding from various parts of the body (including nose, mouth and gums or skin bruising); severe continuous abdominal pain mainly due to enlarged liver, and shock in severe cases. This can lead to death. DHF is more serious in children. According to data from epidemiology unit of Sri Lanka; most affected districts were Kandy, Colombo, Gampaha and Kaluthara. These districts which have been susceptible in the past have recorded a high rate of infection and deaths.
Patients become infected once bitten by mosquitos. The virus passes to lymph nodes and replicates which is followed by spread to the circulation and other tissues. It is thought that in
fection with a secondary serotype is what leads to severe hemorrhagic disease. Disease varies in severity. Incubation period is 2-7 days. All hemorrhagic fever syndromes begin with abrupt onset of fever (39,5-41 °C) and myalgia. Fever is often biphasic with two peaks. Fever is associated with frontal or retro-orbital headache lasting 1 -7 days, accompanied by generalized macular, blanching rash. Initial rash usually fades after 1 -2 days. Symptoms regress for a day or two then rashes reappear in maculopapular, morbilliform pattern, sparing palms and soles of feet. Fever recurs but not as high. There may be desquamation. DF cases experience severe bony and myalgic pain in legs; joints and lower back which may last for weeks (hence break bone fever). Nausea, vomiting, cutaneous hyper aesthesia, taste disturbance and anorexia are common. Abdominal pain may occur and if severe suggests DHF pattern. The signs of dengue fever/ dengue hemorrhagic fever are — high fever, rash, hypotension and narrow pulse pressure, poor capillary refill. There may be hepatomegaly and lymphadenopathy. A tourniquet placed on an arm may induce petechiae in early DHF cases.
DHF sufferers exhibit a bleeding tendency as evidenced by petechiae, purpura, epistaxis, gum bleeding, GI hemorrhage and menorrhagia. There may be pleural effusion, ascites and pericarditis due to plasma leakage. Petechiae are best visualized in the axillae. Flushing of head and neck. Tender muscles on palpation. Periorbital oedema and proteinuria may be present. Maculopathy and retinal hemorrhages may also occur. DSS pattern cases progress through DHF until profound shock due to severe hypotension is present. Symptoms range from a mild fever, to incapacitating high fever, with severe headache, pain behind the eyes, muscle and joint pain, and rash. DHF is a potentially lethal complication, affecting mainly children. There are no specific antiviral medicines for dengue. It is important to maintain hydration. Use of acetylsalicylic acid (e.g. aspirin) and non steroidal anti-inflammatory drugs (e.g. Ibuprofen) is not recommended. The public is advised to seek medical attention at the nearest hospital since early clinical diagnosis and careful clinical management by experienced physicians and nurses increase survival of patients.Exclusion from childcare, preschool, school or work is usually not necessary but people experiencing fever from dengue infection should not be in an environment where they may be bitten by mosquitoes. If this is not possible they should stay at home until they have no fever and are therefore no longer infectious (usually 3 to 5 days).
There is no vaccine to prevent human infection by this virus and it is still being researched.
There is a bacterium called Bacillus thuringiensis which contains spores that produce toxins that specifically target and only affect mosquito larvae and there have been national level researches which are being carried out to use this bacteria Bacillus thuringiensis in order to destroy mosquito larvae [2].
Personal protection and the environmental management of mosquitoes are important in preventing illness.
Anti-mosquito public health measures such as reducing breeding sites (flower pots, fish tanks, tires, coconut shells, tins, water collecting plants, gutters which can collect water) and good sewage management. Insecticides to destroy the larvae. Mosquito nets can be used during day time as the Aedes mosquitoes are day-biting. Use mosquito repellents.Prevent access of mosquitoes to an infected person with a fever.
Protect yourself from mosquito bites at all times especially in areas where dengue is spread. The aim
To give a territorial-temporal characterization of the incidence of dengue fever in Sri Lanka and evaluate the effectiveness of the organization of treatment and preventive measures.
Material and research methods
We analyzed literature and statistical data on dengue fever cases in Sri Lanka. Through the analysis we were able to brief the management and preventive measures that are applied in Sri Lanka.
Research results and discussion
The population of Sri Lanka is 20.97 million (2015) people. Some 1.84 million are migrant workers. The number of Dengue Fever affected individuals in 2015 was 29777. In 2016 it was 55154. Statistics for the first 5 months of 2017 show affected individuals as 56,887. And the total number of dengue affected individuals rose to more than 186000. Following the above mentioned statistics, the simple mathematical calculation gives an alarming figure of the percentage of dengue affected individuals to date. It is approximately 1 % of the entire population for the period of three years, 2015-2017. In 2018, dengue fever in Sri Lanka infected more than 51000 people; 50 people died. The number of people infected with dengue fever in Sri Lanka since the beginning of the 2019 year has exceeded 58000 people; more than 70 people have died, citing data from the country's Epidemiological Department [1], (Picture 1).
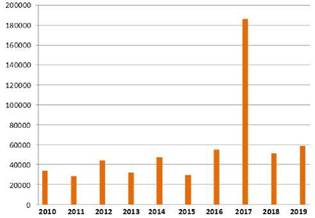
Picture 1 — Reported dengue cases per year since 2010-2019
It is noted that up to this date, almost 58680 thousand cases of the disease were recorded, most of all-in the Metropolitan district of Colombo (about 11.8 thousand infected).
In addition, experts stressed that there are five districts in the country where there is an increased risk of contracting the fever virus: the Metropolitan district of Colombo, the districts of Gampaha and Kalutara in the Western province, the district of Galle-in the South, and the district of Ratnapura in the South east of the island.Dengue fever is most common in children and middle — aged and elderly people, but up to half of the deaths occur in adults aged 20 to 40 years. Local Government Institutions play a major role in the Dengue Prevention Scheme. There is a severe outcry by the people about the total collapse of the State's mechanism on Dengue Fever Prevention. Refer picture 2.
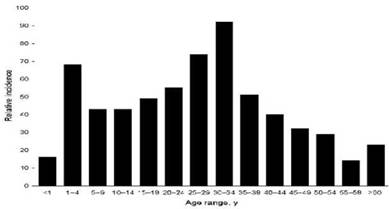
Picture 2 — Dengue epidemic distribution amongst different age groups of Sri Lanka
Conclusions
The outbreak situation in 2017 warranted extensive and regular removal of possible mosquito breeding sites from the environment, along with strengthened patient education on management of fever which resulted in a relatively low mortality. It is very important to seek medical attention in the event of fever and to do relevant laboratory investigations at least by day three of the illness and the citizens have been informed regarding this fact. According to the reveals of laboratory investigations there have been a prototype findings such as FBC — low platelets and high packed cell volume if haemoconcentrated. Usually white cell count will fall. Infection may be confirmed by isolation of virus in serum and detection of IgM and IgG antibodies for Dengue by ELISA, monoclonal antibody or haemagglutination. Molecular diagnostic methods such as reverse-transcriptase-PCR are increasingly being used. Chest X-ray may show pleural effusion.
Literatura
1. National Dengue Control Unit, Sri Lanka. — 2019.
2. Epidemiology Unit of Ministry of Health, Sri Lanka. — 2010.
3. World Health Organization/ Emergency Preparedness, Response/ Dengue Fever- Sri Lanka (2010-2017).
4. The global distribution and burden of dengue / S. Bhatt [et al.] // Nature. — 2010. — Vol. 496. — P. 504-507.
5. Refining the global spatial limits of dengue virus transmission by evidence-based consensus / O. J. Brady [et al.] // PLoS Negl Trop Dis. — 2012. — Vol. 6. — P. 1760.
Еще по теме DENGUE FEVER: OVERVIEW OF MEDICAL ACTIVITIES IN SRI LANKA:
- Chapter 1. Clinical trials of medicines for medical use as the means of implementation of the state’s social policy
- Chapter 2. Social protection of patients participating in clinical trials of medicinal products for medical use
- Chapter 3. Social protection of a physician-scientist while carrying out clinical trials of medicines for medical use
- HIV STIGMATIZATION AMOUNG MEDICAL STUDENTS: RELATIONSHIP WITH THEIR KNOWLEDGE OF HIV
- General characteristics of social protection and its legal mechanisms for individuals participating in clinical studies of medicines for medical use
- Clinical trials of medicines for medical use as a stage of supply of medicines: concept, participants, features and legislative governance
- General characteristics of approaches as to the construction of legal mechanisms for the social protection of a physician-scientist.
- ДЕНГЕ
- Рекомендации для дальнейшего изучения
- Preventive public law mechanisms of social protection of patients